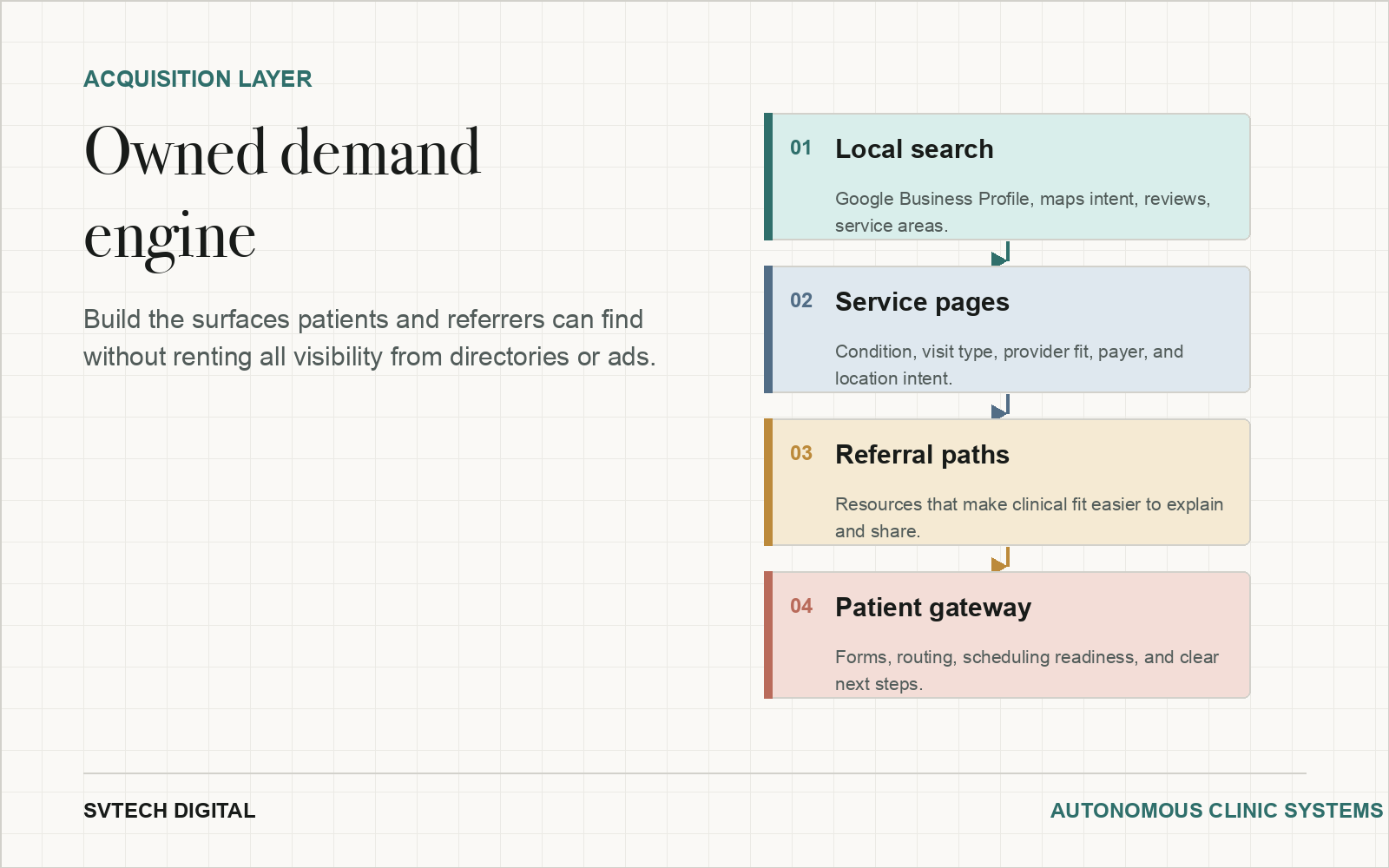
Acquisition-limited practices are too dependent on rented visibility.
Directories, paid ads, and passive referrals can still matter, but they do not build authority the practice keeps. Owned demand comes from local search, service pages, credentialed content, and referral paths that compound.