The model
A five-layer operating system for psychiatric practice growth.
The Autonomous Clinic model starts with owned organic demand, then builds the systems needed to absorb it: patient gateway, practice nervous system, care between visits, and intelligence loops.
System diagram
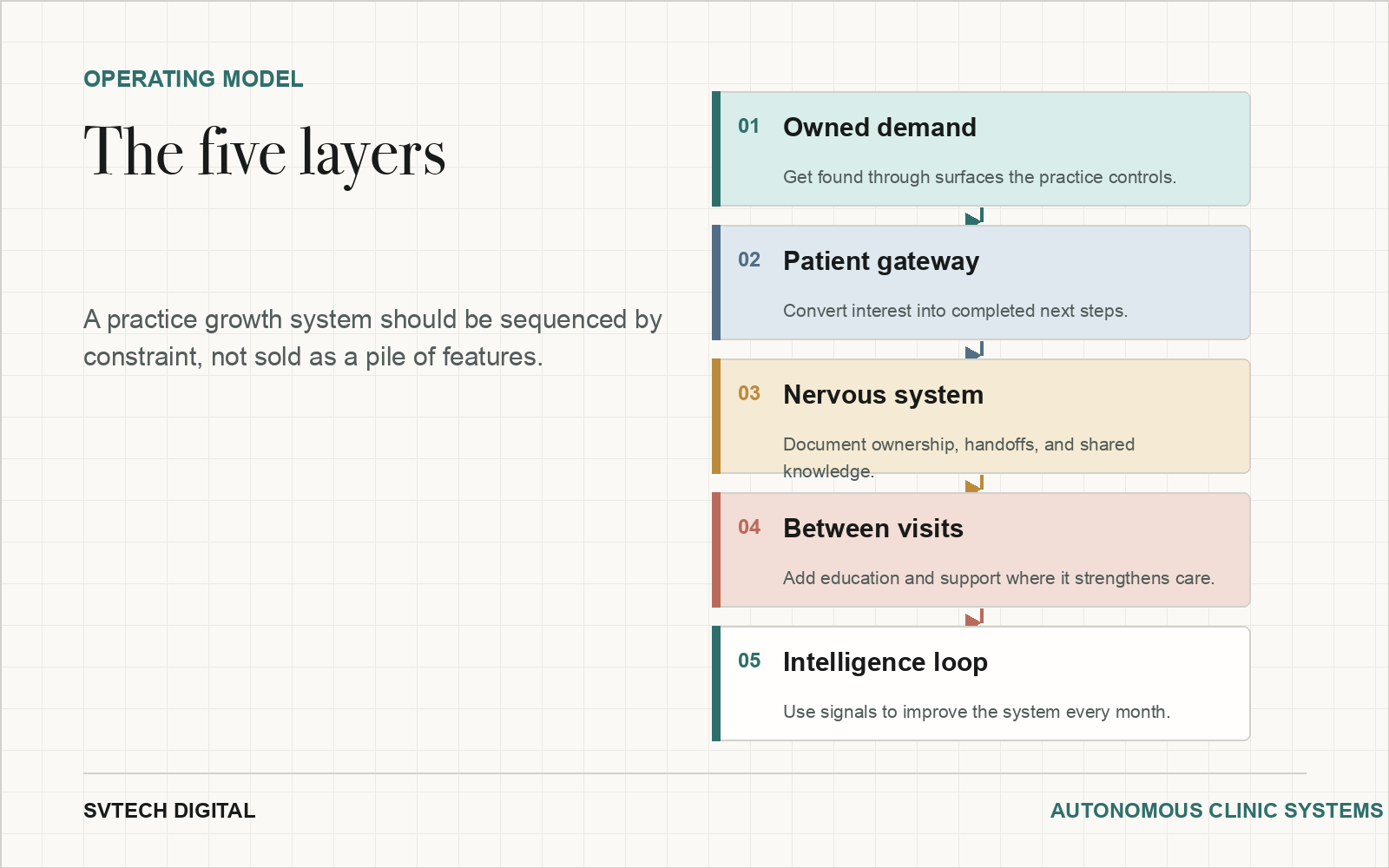
The Autonomous Clinic in five layers.
This diagram turns the manuscript model into a clean visual sequence: owned demand, patient gateway, nervous system, between-visit support, and intelligence loop.
At a glance
The decision in brief.
The five layers
Owned demand creates durable visibility. The patient gateway turns interest into completed next steps. The nervous system reduces staff rework. Between-visit care adds structured support. The intelligence loop turns questions, drop-offs, and outcomes into better decisions.
Why sequence matters
If demand is thin, automation alone does not create patients. If intake is leaking, more traffic creates more chaos. If operations are undocumented, growth depends on memory instead of infrastructure.
What to measure
Track organic clicks, service-line inquiries, form starts, completed intake packets, booked visits, response time, no-shows, staff touches, patient questions, and content gaps.
Key system elements.
Each element connects a common practice constraint to a concrete operating response.
Manuscript depth
Why the model starts with owned demand but does not stop there.
The manuscript is blunt about the mistake most independent psychiatric and behavioral health practices make: they treat acquisition, intake, operations, education, and analytics as separate purchases. A directory listing sits in one bucket. A form tool sits in another. Staff messaging sits in another. Patient education sits somewhere else entirely. The owner then tries to judge each item by its monthly cost instead of asking what system the practice is actually building.
The Autonomous Clinic model reframes the work as an operating system. Owned demand is first because a practice that cannot be found by the right patients is dependent on rented visibility. Directories and ads may remain useful, but they should not be the only source of truth. The practice needs searchable, credentialed, local, service-line, and referral-aware surfaces it controls. Those surfaces become more valuable when they compound over time.
The patient gateway comes next because more visibility can hurt a practice whose intake path is already overloaded. When forms, calls, eligibility questions, scheduling, consent documents, reminders, and handoffs are scattered, every new inquiry adds work. A better gateway does not remove clinical judgment. It reduces avoidable friction before clinical judgment is needed.
The practice nervous system is the layer most owners under-value. It is the written and shared operating knowledge that keeps the practice from depending on one person's memory. Intake rules, staff ownership, response standards, exceptions, onboarding steps, and recurring decisions need a place to live. Without that layer, growth creates more meetings, more interruptions, and more invisible work.
Between-visit care and patient education belong later in the sequence. They can be powerful when the practice already understands its demand, gateway, and workflow constraints. They become dangerous when used as a vague promise that technology will extend care without governance. The right question is not whether a practice can add education, check-ins, or a platform. The right question is where those supports strengthen care, retention, readiness, and clinical visibility without pretending to replace treatment.
The intelligence loop is what turns the whole system into an asset. Search queries show what patients are trying to understand. Intake drop-offs show where the gateway is confusing. Repeated staff questions show where the nervous system is incomplete. No-shows and incomplete forms show where readiness is weak. Patient education engagement shows where support is useful and where it is not. A practice that reviews those signals monthly learns faster than a practice that only buys more tools.
How to choose the first layer.
The model is not meant to make every practice buy every capability. It is meant to stop owners from starting in the wrong place.
Frequently asked questions
Questions this page answers directly.
What is The Autonomous Clinic?
It is a practice operating model that connects owned demand, intake, workflow, between-visit support, and measurement.
Does every practice need all five layers?
No. The first layer should match the constraint. Some practices need organic demand first; others need intake or workflow repair.
Is this a software product?
No. It is a build sequence. Software may be part of the implementation, but the model starts with the practice bottleneck.
Next step
Map the constraint before buying more tactics.
The first recommendation should identify whether the practice needs owned demand, a better patient gateway, internal workflow, care support, measurement, or a sequenced combination.