Search intent: AI front desk psychiatry. This guide is written for owners and clinical directors who need practical systems rather than marketing slogans.
Source-informed from manuscript Chapter 9: AI front desk, crisis-escalation boundary, TCPA/HIPAA/state-law layers, and fail-closed routing.
The answer in one paragraph
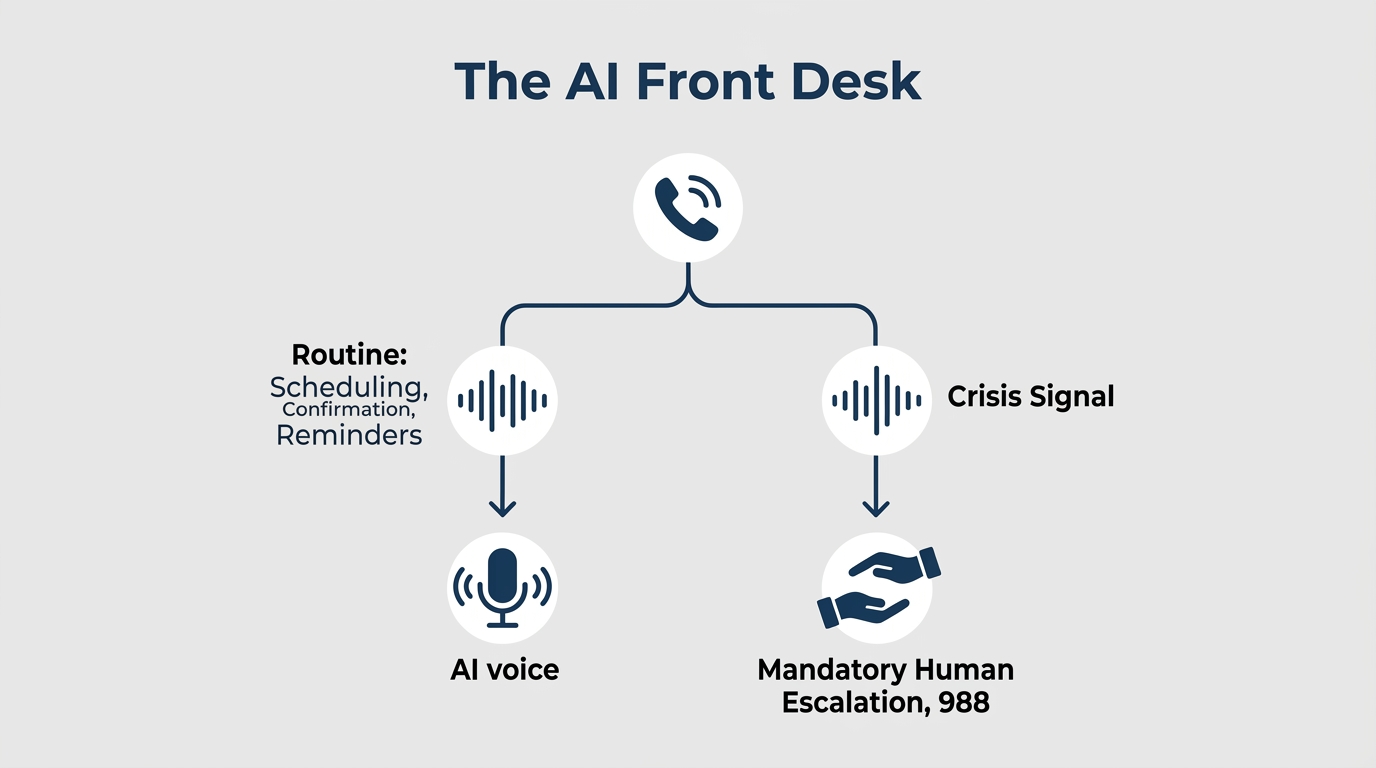
An AI front desk for psychiatry should handle narrow administrative work: answering basic questions, capturing inquiry details, scheduling or routing, reminders, and rescheduling. It should not diagnose, triage crises independently, discuss treatment decisions, or pretend to be a clinician. The safe architecture is administrative automation with human escalation built in.
The boundary that matters
The manuscript draws a bright line: an AI system can recognize defined risk indicators and escalate, but it should not be described as reliably detecting a crisis. That difference changes how staff trust the system. If a caller mentions self-harm, acute danger, medication emergencies, or ambiguous risk language, the automated flow should stop and route to a human or crisis resource.
Compliance is layered
Three layers matter before deployment: HIPAA and BAA coverage for any PHI, TCPA consent and opt-out requirements for outbound AI voice calls, and state-specific healthcare AI disclosure rules that are changing quickly. A psychiatric practice should document those answers before a live deployment, not after the first strange call.
Where AI front desk helps
The useful lane is repetitive administrative volume: after-hours inquiry capture, appointment confirmation, rescheduling, basic practice policy questions, and structured routing into intake. This can reduce staff interruption and help the practice respond faster without expanding the front desk.
Implementation checklist
- Define exactly what the AI may and may not answer.
- Test crisis and ambiguity scenarios before launch.
- Confirm BAA coverage in writing.
- Document outbound-call consent and opt-out rules.
- Review transcripts and escalation accuracy regularly.
Frequently asked questions
Can an AI front desk handle psychiatric crisis calls?
It should escalate crisis indicators; it should not independently manage or resolve a crisis.
Should patients be told they are speaking with AI?
Yes. Disclosure is both ethically cleaner and increasingly important legally.
What is the safest first use case?
After-hours inquiry capture and scheduling support with human review is usually safer than open-ended clinical conversation.