The answer in one paragraph
A psychiatric patient intake workflow should collect the right information once, carry it forward, route the patient clearly, complete forms and signatures before the first visit, and show staff what is missing. Automation should reduce repetition and confusion while preserving human review for fit, risk, and clinical judgment.
Where intake leaks
Practices lose patients when calls, forms, insurance fit, scheduling, reminders, signatures, and handoffs sit in separate places. The patient sees repetition. Staff see another chase list. The owner sees volume without clarity.
What to build first
Map the current path from inquiry to first appointment. Remove duplicate entry. Add a structured form, signature flow, readiness questions, reminder rhythm, and staff routing. Then track inquiry-to-completed-intake time.
What to measure
Measure form completion, time to completion, response speed, no-show rate, missing information, staff touches, and booked appointments by source.
Why intake automation is not just convenience
In psychiatric practices, intake is where acquisition becomes either care or waste. A person can find the practice through organic search, a referral, a directory, or word of mouth, but that demand only becomes valuable if the next steps are clear. If calls go unanswered, forms repeat information, signatures are missing, insurance questions require multiple follow-ups, and scheduling requires manual chasing, the practice loses momentum before care begins.
Automation should reduce the avoidable work around that path. It should not make clinical decisions, screen out ambiguity without human review, or pretend every patient can be routed by a form alone. Good automation collects information once, carries it forward, shows staff what is missing, and gives the patient a clear sense of what happens next.
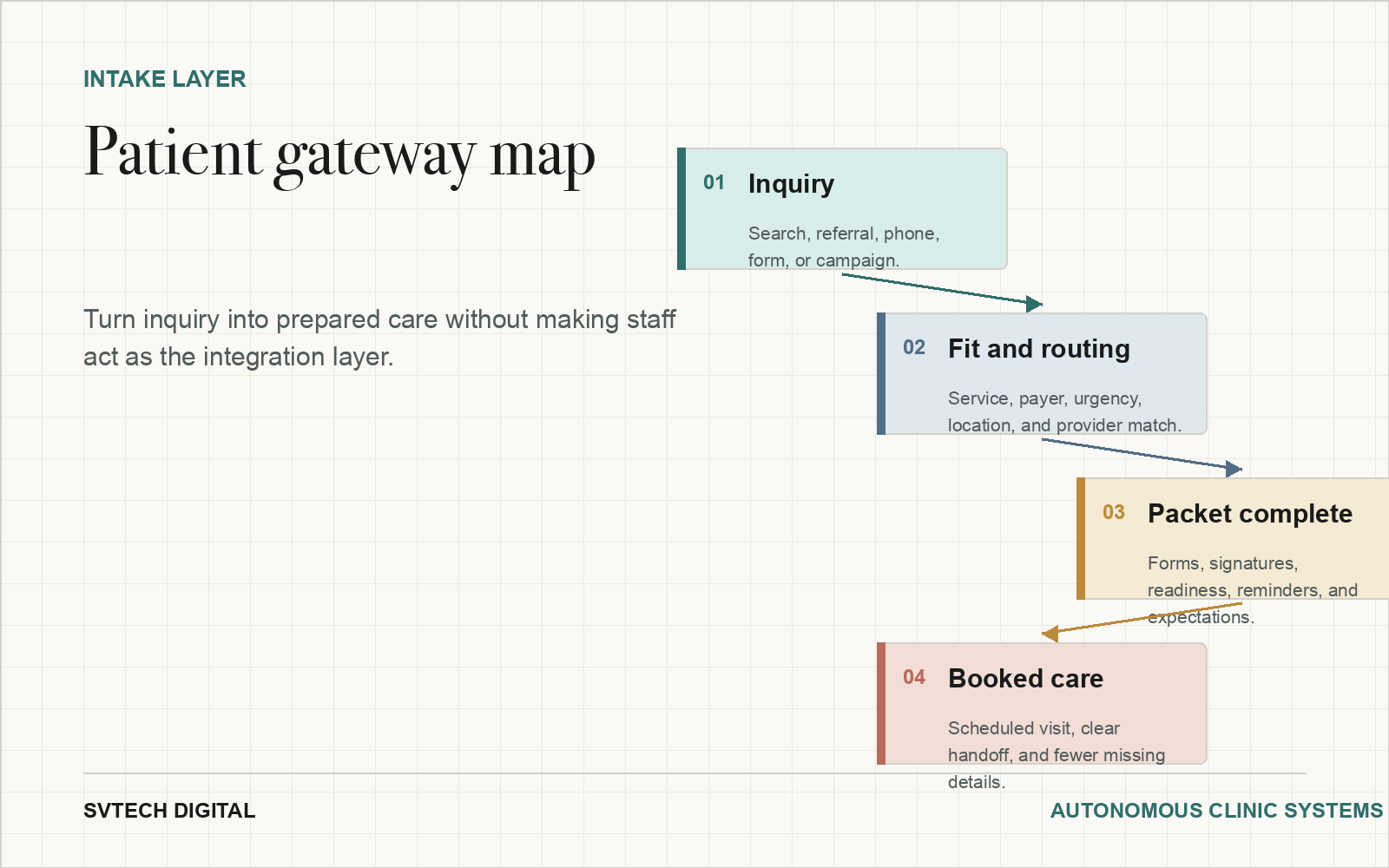
The patient gateway map
Start by mapping the path from inquiry to first appointment. Where does the inquiry originate? What form or call captures it? How does staff know who owns the next step? What questions determine fit, payer, urgency, location, modality, provider match, and readiness? Where do signatures happen? What reminders are sent? What does the patient receive before the first visit?
Most leaks appear when those steps live in separate places. A website form creates one record. A phone call creates a note. A scheduling tool creates an appointment. A signature tool creates a document. The EHR contains another version of the story. Staff become the integration layer. The goal of the gateway is to reduce that invisible staff burden.
What to automate first
The first automation should target the highest-friction step. For many practices, that is paperwork completion and signature collection. For others, it is response time, eligibility capture, appointment-readiness questions, reminder rhythm, or handoff from inquiry to scheduling. The starting point should come from real data and staff interviews, not from a vendor demo.
A practical first build might include a structured inquiry form, conditional questions, confirmation email, staff notification, e-signature packet, reminder sequence, and a simple status view showing new inquiry, needs response, packet sent, packet complete, consult scheduled, first visit scheduled, and stalled. That is often enough to create visible relief.
Compliance and clinical boundaries
Psychiatric practices need to be careful about tools that handle protected health information. Business associate agreements, data settings, retention policies, access control, and form configuration matter. A vendor saying it supports healthcare is not the same as the practice having the correct agreement and workflow in place.
Clinical boundaries matter too. Intake automation can collect information and route next steps. It should escalate urgent language, unclear fit, crisis indicators, or sensitive exceptions to a human. The practice should decide where automation stops before a patient enters the system.
What to measure after launch
Track average time from inquiry to first response, form start to completion, packet completion, scheduled consults, first appointments, no-shows, missing information, staff touches, and source-level conversion. If organic demand is increasing but completed intakes are not, the gateway still has friction. If completed intakes increase but booked visits do not, scheduling or fit may be the constraint.
These numbers should feed the practice intelligence loop. Intake questions can reveal content gaps. Missing information can reveal form design problems. Slow completion can reveal unclear patient instructions. Staff exceptions can reveal where routing rules need to improve.
Related SVTech Digital resources
For the complete model, read The Autonomous Clinic model. For service options, review lead capture, scheduling, and onboarding services. For measurement, read the practice intelligence loop guide.
Where automation should hand off to humans
The cleanest intake systems include human review points by design. Fit decisions, safety concerns, complex medication histories, controlled-substance questions, crisis language, unclear insurance issues, and unusual scheduling needs should not disappear into a workflow queue without ownership. Automation should make those exceptions more visible, not less.
A practical rule is to automate clarity and escalate ambiguity. If the next step is predictable, automate the reminder, form, confirmation, or routing. If the next step requires judgment, make sure the right person sees it quickly with enough context to respond. This balance is especially important in psychiatric care because the first interaction can contain clinically meaningful information.
Good patient gateway design also protects staff. It reduces repeated explanations, duplicate data entry, and unclear ownership. Staff should not have to remember which patient needs which document, which call needs follow-up, or which intake is stalled. The workflow should show that.
Gateway visual
Intake automation should clarify the path.
Track inquiry, fit routing, packet completion, and booked care as one visible patient pathway.
How to measure the work
Frequently asked questions
What should not be automated?
Clinical judgment, crisis response, and ambiguous fit decisions should route to a human.
Does intake automation require EHR integration?
Direct integration helps, but structured intake can still reduce work even when a manual transfer remains.
What is a good first goal?
A clean first goal is a faster completed intake packet with fewer staff touches and clearer patient next steps.